- Details
- ICNA
- News
- Hits: 768
A systematic review of the evidence confirms that infection with mosquito-borne Zika virus is a cause of Guillain-Barre Syndrome (GBS), in addition to microcephaly and other congenital brain abnormalities, according to a study published in PLOS Medicine by Nicola Low of the University of Bern, Switzerland, and colleagues in the World Health Organization (WHO) Zika Causality Working Group.
In March 2016, WHO stated that there was a strong scientific consensus that Zika virus is a cause of GBS, microcephaly, and other neurological disorders. However, decisions about causality must be assessed systematically to guide public health actions. In the new work, the WHO group defined specific questions about the relationship between Zika virus and clinical outcomes, setting a framework of ten dimensions to define causality. They then reviewed existing literature for studies that addressed the outcomes - either GBS or congenital brain abnormalities - and convened a panel of experts to assess the review findings.
Based on 72 studies published up to May 30, 2016, that included data on Zika and congenital brain abnormalities, the team concluded that at least eight of the ten criteria for causality were met. Based on 36 studies published in the same time frame with data on Zika and GBS, the researchers concluded that at least seven of the ten criteria for causality were met. In addition, papers published after the initial literature review - between May 30 and July 29, 2016 - strengthened the initial findings that Zika virus is causative of brain abnormalities and GBS.
Rapid and systematic reviews with frequent updating and open disseminating are now needed, both for appraisal of the evidence about Zika virus infection and for the next public health threats that will emerge
However, there are remaining questions about the link that will need to be addressed with continuing studies. The review was funded by the World Health Organization (http://www.who.int/en/, contract numbers 2016/611294-0 and 2016/630126-0 awarded to NL) and the Swiss National Science Foundation (www.snf.ch, SNSF special action fund and project grant 320030_170069 awarded to NL). The WHO Zika Causality Working Group was involved in interpretation of the data and the decision to publish.
Article: Zika Virus Infection as a Cause of Congenital Brain Abnormalities and Guillain-Barré Syndrome: Systematic Review, Krauer F, Riesen M, Reveiz L, Oladapo OT, Martínez-Vega R, Porgo TV, et al., PLOS Medicine, doi: 10.1371/journal.pmed.1002203, published 3 January 2016...
Read More
- Details
- ICNA
- News
- Hits: 811

SPINRAZA (nusinersen) is an antisense oligonucleotide (ASO) that is designed to treat SMA caused by mutations in the chromosome 5q that leads to SMN protein deficiency. SPINRAZA (nusinersen) alters the splicing of SMN2 pre-mRNA in order to increase production of full-length SMN protein. ASOs are short synthetic strings of nucleotides designed to selectively bind to target RNA and regulate gene expression. Through use of this technology, SPINRAZA (nusinersen) has the potential to increase the amount of full-length SMN protein in patients with SMA.
SPINRAZA (nusinersen) is administered via intrathecal injection, which delivers therapies directly to the cerebrospinal fluid (CSF) around the spinal cord, where motor neurons degenerate in patients with SMA due to insufficient levels of SMN protein.
The most common adverse reactions reported for SPINRAZA (nusinersen) were upper respiratory infection, lower respiratory infection and constipation. Serious adverse reactions of atelectasis were more frequent in SPINRAZA (nusinersen)-treated patients. Coagulation abnormalities and thrombocytopenia, including acute severe thrombocytopenia, have been observed after administration of some antisense oligonucleotides.
Renal toxicity, including potentially fatal glomerulonephritis, has been observed after administration of some antisense oligonucleotides.
SMA360°
Surrounding you with support
Read More
- Details
- ICNA
- News
- Hits: 798
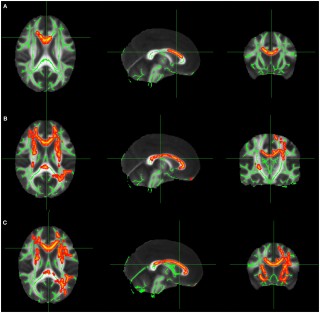
In research presented at the 2016 American Epilepsy Society annual meeting in Houston University of Munich Hospital's epilepsy center and its department of neuroradiology reported on their findings from using DTI to locate epileptogenic abnormalities. The technique is already being regularly used to guide implantation of intracranial electrodes at the University of Munich. The DTI technique involves quantification of regional U-fibers to identify microstructural abnormalities in patients with cryptogenic focal epilepsy (cFE).
The most frequent pathology in cases with cryptogenic focal epilepsy is focal cortical dysplasia, which is typically located at the gray-white-matter border, typically in the bottom of a sulcus, and this is where U-fibers are located. The density of U-fibers we analyzed is therefore a specific neuroimaging biomarker for the gray-white-matter border and seems to be very sensitive to alterations caused by subtle forms of focal cortical dysplasia.
They studied 55 cFE patients and 60 healthy controls. Whole-brain tractography by DTI was performed, and tracts representing subcortical U-fibers were selected based on length, curvature, and shape. Tract density images were then created, specifying the number of tracts passing through any voxel. Clusters of significant reductions in U-fiber density were compared with clinical data from presurgical evaluation, including ictal and interictal electroencephalography (EEG), seizure semiology, fluorodeoxyglucose-positron emission tomography (FDG-PET), and ictal single-photon emission computed tomography imaging (SPECT).
Finaly analysis was done on 43 patients where detailed clinical data was available, clusters of significant U-fiber reductions were found in 91 percent of the patients, and 78 percent were consistent with the clinical localization of the epileptogenic zone. Twelve patients underwent intracranial EEG recording with depth electrodes, confirming seizure onset in 74 percent of the detected U-fiber reductions. Eight patients had resective surgery, and the most frequent histopathologic finding was mild malformation of cortical development, with blurred gray-white matter border and ectopic neurons in the white matter.
According to Christian Vollmar, MD, PhD at the University of Munich, U-fiber quantification is definitely good enough to base further investigations on, particularly to plan the implantation of invasive electrodes, and to give it the same weight that other established methods like ictal SPECT or FDG-PET. No single diagnostic modality alone is ever good enough to base surgical decisions on in case of cryptogenic focal epilepsy." It is important to note that this report requires validation in larger, prospective studies, with outcome data to substantiate whether the technique ultimately results in fewer seizures following surgery. In addition it also relies on accurate DTI mapping with the parameters set in just the right way.
- AES Abstract 3.196: Vollmar C, Goc J, Hartl E, Noachtar S. U-fiber track density imaging identifies specific alterations in the epileptogenic zone in individual patients with cryptogenic focal epilepsy.
- Just pretty pictures? What diffusion tractography can add in clinical neuroscience - Heidi Johansen-Berg and Timothy E.J. Behrens
Read More

- Details
- ICNA
- News
- Hits: 923
Ich bin schon ein toller Typ (I am already a great guy)
Dieter Janz himself joked when he addressed the guests at his 90th birthday celebrations : "After all that I have heard about myself today, I must say: I am already a great guy" - impressed by himself after all the praise , And especially thanked his wife Gabriele for 62 common years of marriage.
Akademische Feier zum 90. Geburtstag des Epileptologen Professor Dieter Janz, Emeritus der Freien Universität
Read More
- Details
- ICNA
- News
- Hits: 840
Dear colleagues,
We are writing today to ask for your support for the International Child Neurology Association (ICNA) and its activities. http://www.icnapedia.org
The work that ICNA performs is entirely financed from funds raised. Membership is now free and has grown considerably to over 2,000 members since we implemented this policy in 2012.
Strategic aims of the ICNA
- Helping and supporting colleagues from resource poor regions to elevate standards in the clinical practice of child neurology and neurodisability internationally.
- ICNA has ambitious plans to advance this cause through increased educational programs in resource poor countries.
- The International Child Neurology biennial congresses (ICNC) are on track. These academic meetings are greatly valued for their state-of-the-art scientific content and interactive educational workshops and have been highly successful over the years. Following a landmark clinical, scientific and educational ICNA congress in 2016 in Amsterdam, we are looking forward to our next ICNA Congress, Nov. 15-18th, 2018 in enchanting Mumbai, India. Our congress theme will focus on “Protecting the developing brain and preventing disability”. Please mark your calenders for this event as we will shortly be sending out a call for the submission of competitive symposia.
- An open access free electronic journal (JICNA) has been recently launched (editor Charles Newton) and there is continued expansion of online resources on our website ICNApedia including online lectures, guidelines, WHO alerts, clinical videos, neuroimages, journal watch, fellowship and research grant opportunities including our global burden of disease seed grant fellowships, etc.
The educational programs of ICNA in 2016 were enormously successful with 18 meetings across the globe, which is the highest annual number to date. The countries included Bangladesh, Barbados, Brazil (4 sites), Colombia, Egypt, India (3 sites), Iran, Italy, Jamaica, Myanmar, Russia, Tanzania, and Zimbabwe, illustrating the aim of ICNA to try and ensure global reach.
The feedback from participants has been highly positive as were the clinical and scientific interactions. ICNA board members as well as general ICNA members donated both their time and their expertise as well as in the large part supporting their own travel to meeting sites, which underlines the true beneficence of our members and our mission.
We would like to specifically acknowledge the efforts of our 2016 meeting organizers namely Banu Anlar (Turkey), Ana Carolina Coan (Brazil), Paolo Curatolo (Italy), Marilisa Guerreiro (Brazil), Ahmed Raouf Ibrahim (Egypt), Sakkubai Naidu (USA), Pratibha Singhi (India), Ingrid Tein (Canada), Sylvia Tenembaum (Argentina), Vanessa Van der Linden (Brazil), and Jo Wilmshurst (South Africa).
A public health emergency has been recognized by the WHO and PAHO arising from the mosquito-borne ZIKA virus which is leading to an endemic disease of profound congenital microcephaly with severe developmental disability, seizures, blindness, spasticity, and deafness as well as acquired transverse myelitis and Guillain-Barre syndrome in the Southern hemisphere and moving toward the Northern hemisphere. ICNA designed and delivered a series of ZIKV educational symposia to heighten awareness of the clinical recognition, diagnosis, management and prevention of ZIKV associated morbidity and mortality.
These workshops held in Brazil (Recife, Campinas, Sao Paolo, Iguazus), Colombia (Bogota) and the Netherlands (ICNC2016, Amsterdam) were highly successful in disseminating critical up-to-date information and WHO guidelines internationally, as well as in high endemic regions to over 2,700 health practictioners many of whom were/are directly in the front-line. We are extremely grateful for the hardworking and steadfast efforts of our ICNA-ZIKV working group members (Vanessa Van der Linden, Marilisa Guerreiro, Ana Carolina Coan, Helen Cross (UK), Jo Wilmshurst, Charles Newton (Kenya, UK), Ingrid Tein).
One of the new aspects of the ICNA educational mission has been to partner in several instances with the International Committee of the Child Neurology Society (CNS) in the USA. This committee is headed by Jorge Vidaurre, a Spanish-speaking epileptologist from Nationwide Children’s Hospital in Columbus, Ohio. We have obtained a small budget from the CNS for certain joint ventures. Since 2015, we have had joint meetings with the CNS in Bolivia, Honduras, Tanzania, and Zimbabwe and have endeavoured to have Spanish-speaking faculty whenever appropriate.
ICNA has also aligned its goals in reducing the global burden of neurologic diseases associated with intellectual disability, epilepsy and traumatic brain injury with the World Federation of Neurology and as a member of the World Brain Alliance. Through the WBA, we are advocating for recognition of Brain Non-Communicable Diseases by the WHO and for support from governmental, social and public sectors to prevent, reduce and/or modify the exponentially increasing human and financial cost of all neurodegenerative disorders.
As we are about to embark into a new year of promises and aspirations to benefit and maximize the potential of children in all corners of the world, we are reaching out for your valued support. Please consider making a donation to ICNA. No amount is too small! As an international group, we expect donations to be highly variable in the amount. It is perfectly OK to donate US $25 (or more) and be listed as a donor on the ICNA website. This support will fund more critically needed educational meetings in resource-poor regions. Every dollar goes directly toward education and makes a synapse in our network between resource-rich and resource-poor regions. We truly need this support!
Please visit the ICNA webportal at http://www.icnapedia.org to make your donation. If possible, we prefer not to have paper checks because of excessive bank charges. We will be happy to provide you with a letter of thanks acknowledging your donation.
We sincerely thank you and extend to you and your family our best wishes for the holiday season and for a very joyful, peaceful and prosperous 2017.
Read More