
In research presented at the 2016 American Epilepsy Society annual meeting in Houston University of Munich Hospital's epilepsy center and its department of neuroradiology reported on their findings from using DTI to locate epileptogenic abnormalities. The technique is already being regularly used to guide implantation of intracranial electrodes at the University of Munich. The DTI technique involves quantification of regional U-fibers to identify microstructural abnormalities in patients with cryptogenic focal epilepsy (cFE).
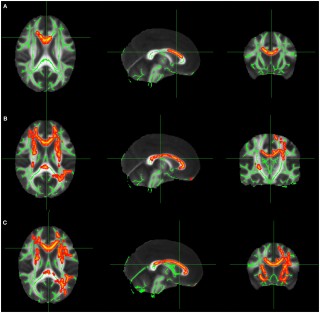
The most frequent pathology in cases with cryptogenic focal epilepsy is focal cortical dysplasia, which is typically located at the gray-white-matter border, typically in the bottom of a sulcus, and this is where U-fibers are located. The density of U-fibers we analyzed is therefore a specific neuroimaging biomarker for the gray-white-matter border and seems to be very sensitive to alterations caused by subtle forms of focal cortical dysplasia.
They studied 55 cFE patients and 60 healthy controls. Whole-brain tractography by DTI was performed, and tracts representing subcortical U-fibers were selected based on length, curvature, and shape. Tract density images were then created, specifying the number of tracts passing through any voxel. Clusters of significant reductions in U-fiber density were compared with clinical data from presurgical evaluation, including ictal and interictal electroencephalography (EEG), seizure semiology, fluorodeoxyglucose-positron emission tomography (FDG-PET), and ictal single-photon emission computed tomography imaging (SPECT).
Finaly analysis was done on 43 patients where detailed clinical data was available, clusters of significant U-fiber reductions were found in 91 percent of the patients, and 78 percent were consistent with the clinical localization of the epileptogenic zone. Twelve patients underwent intracranial EEG recording with depth electrodes, confirming seizure onset in 74 percent of the detected U-fiber reductions. Eight patients had resective surgery, and the most frequent histopathologic finding was mild malformation of cortical development, with blurred gray-white matter border and ectopic neurons in the white matter.
According to Christian Vollmar, MD, PhD at the University of Munich, U-fiber quantification is definitely good enough to base further investigations on, particularly to plan the implantation of invasive electrodes, and to give it the same weight that other established methods like ictal SPECT or FDG-PET. No single diagnostic modality alone is ever good enough to base surgical decisions on in case of cryptogenic focal epilepsy." It is important to note that this report requires validation in larger, prospective studies, with outcome data to substantiate whether the technique ultimately results in fewer seizures following surgery. In addition it also relies on accurate DTI mapping with the parameters set in just the right way.
- AES Abstract 3.196: Vollmar C, Goc J, Hartl E, Noachtar S. U-fiber track density imaging identifies specific alterations in the epileptogenic zone in individual patients with cryptogenic focal epilepsy.
- Just pretty pictures? What diffusion tractography can add in clinical neuroscience - Heidi Johansen-Berg and Timothy E.J. Behrens
Read More